A Harm Reduction Community of Practice led by Lili Berescu and Priyanka Jani brought the proposal of best practice reductions in wound care forward to the Nurses Specialized in Wound, Ostomy and Continence Canada Board. This case study reflects on the development of the Canadian Best Practice Recommendations on Wound Care in People Who Use Drugs: A Harm Reduction Approach.
These newly published best practice recommendations represent a multi-year collaboration among NSWOCC, the Harm Reduction Nurses Association (HRNA), and the Ontario Network People Who Use Drugs (ONPUD). It was an educational journey for all those involved. The inclusion of people who use drugs in the task force (PWUD) broke important new ground and reflects the real-world experiences of this often stigmatized population. The vision was also to create best practice recommendations that embody the sensitivity of the topic and the creativity of PWUD, with a look and feel that is removed from starchy, conventional clinical guidelines. The choice of purple also sought to reflect the recognized association with the harm reduction community.
The harm reduction approach continues to evolve. Sometimes forwards and sometimes backwards, reflecting societal and political pressures. After publication, I interviewed co-lead Lili Berescu at the 2026 WCET-NSWOCC Joint Congress in Vancouver.
Lili Berescu (they/them), BScN, RN, NSWOC, WOCC(C) – project co-lead.
Harm Reduction Versus Wound Care in PWUD
The project remained a balance between a document on a harm reduction approach to nursing practice and wound care recommendations in PWUD. The twenty-nine members of the task force come from a variety of backgrounds, yet all have a passion and experience with wounds in PWUD.
The 23 recommendations cover the following aspects:
- Social Implications of Criminalization
- Health Systems Approach
- Goals of Wound Care
- Assessment
- Factors of Impaired Wound Healing
- Education and Prevention
- Topical Management of Wounds Related to Substance Use
These best practice recommendations included poems and artwork supplied by PWUD. Modest honoraria were provided to both those who had creative content included and the PWUD who were part of the task force. The document also included a more expansive glossary, similar to those in other NSWOCC projects. Appendix 3 provides QR codes to supplementary resources.
None of us think we got this all right. There was certainly a need for such a resource. Comfort levels varied between empowering PWUD to manage their wounds and supporting their peers. Or should guidance on managing wounds only be made by licenced health care professionals? There is no right or wrong answer. Practices vary by province/territory and may reflect local realities and availability of suitable resources. Everyone involved hopes this is the start of important conversations. We have much to learn by listening to the person in front of us and acknowledging our biases and prejudices.
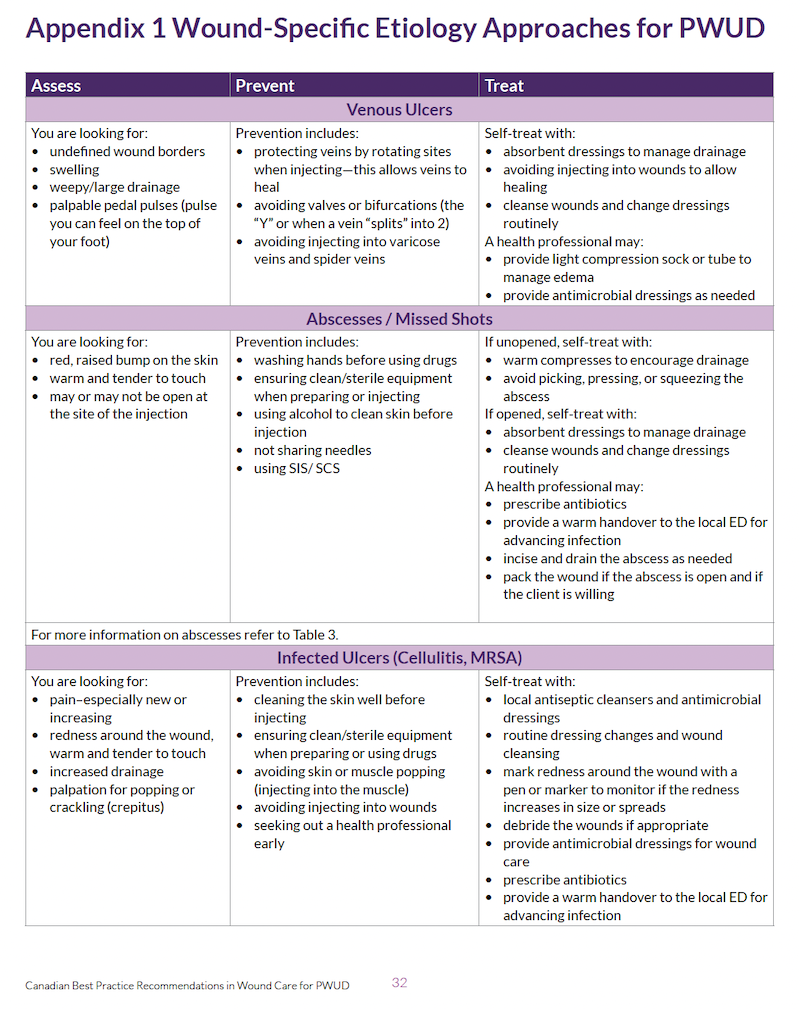
As a central resource, the task force developed Appendix 1. Wound-Specific Etiology Approaches for PWUD. This summarized assessment, prevention, and treatment of five wound etiologies: venous ulcers, abscesses / missed shots, infected ulcers (cellulitis/MRSA), xylazine (nonvasculitis wounds or nonroute specific), and levamisole (induced vasculitis wounds or nonroute specific). The document notes that all health care professionals must abide by federal and provincial/territorial legislation, professional college regulations, and organizational health care setting policies and procedures.
Revisiting the Story Behind the Document Podcast
Members of the task force, Corey Ranger, Andrzej Celinski, Priyanka Jani, and Lili Berescu, explored the story behind the best practice recommendations in a 59-minute podcast episode. The podcast episode offers an opportunity to revisit not just what was created—but why it was created, and how. It can be found on Spotify here.
This podcast captures the intention, care, and collaboration that shaped its development from the very beginning. This work was never intended to be developed quickly. Instead, it was approached with intention—ensuring that all voices were heard, particularly those with lived and living experience, and that the process itself reflected the same harm-reduction principles that the document promotes. The panellists reflect on the time, collaboration, and thoughtfulness required to create guidance that is not only clinically sound but also compassionate, equitable, and grounded in real-world practice.
As Lili Berescue explains in the video interview, politicians and society continue to stigmatize PWUD. Harm reduction approaches have been proven to work yet the Government of Ontario is closing treatment and safe consumption sites. I admire all those advocating to ensure PWUD get all the support services they require.
Thanks to the many individuals who made these new best practice recommendations a success. Thanks to the 35 peer reviewers from Canada and beyond, including members of the Canadian Federation of Mental Health Nurses. A pertinent foreword was supplied by Leigh Chapman (she/elle), PhD, RN, Chief Nursing Officer at Health Canada. Dr. Champan presented at the November 2024 Canadian Pressure Injury Advisory Panel (CPIAP) symposium and shared her nursing background in harm reduction. We thank her for supporting this publication. From my Opencity Inc team, editor Lisa Moulton, clinical nurse researcher Layal Bou Abdo, and graphic designer Deanne Auger. You all did an amazing job of bringing these recommendations to fruition and reflecting the subject matter in a sensitive way.
Many of the project leads for these consensus publications are seasoned health care professionals. This was not the case with Lili and Pri, who were younger nurses with a passion for working with PWUD. They are our future leaders. The development process provided a first exposure to many of the task force members in appraising the literature, Delphi consensus, peer-review, and document editing and production. The Harm Reduction Community of Practice group continues, led by Misty Dawn Stephens, MCISc, RN, FCN, NSWOC, WOCC(C), and Amanda Sowiak, BN, RN, NSWOC, WOCC(C). Among the projects is work on first aid in PWUD and a potential decision aid for nurses in trench foot–a debilitating condition caused by prolonged exposure of the feet to damp, cold, and unsanitary conditions.
Harm Reduction Saves Lives featured image reproduced with permission of Kristi Samuelson.